 I have to admit, I don’t really like flashcards. I especially don’t like it when parents or SLPs use flashcards to drill vocabulary in toddlers and preschoolers, much less school aged children. I feel that it produces very limited learnability and generalization. I am personally a proponent of thematic language learning, since it allows me to take a handful of words/concepts and reinforce them in a number of different ways. The clients still get the benefit of information repetition, much like one would get during a typical flashcard drill. However, they are also getting much more. Thematic language learning allows the client to increase word comprehension, make connections to real life scenarios, develop abstract thinking skills, as well as to transfer and generalize knowledge (Morrow, Pressley, Smith, & Smith, 1997; Ramey, 1995).
I have to admit, I don’t really like flashcards. I especially don’t like it when parents or SLPs use flashcards to drill vocabulary in toddlers and preschoolers, much less school aged children. I feel that it produces very limited learnability and generalization. I am personally a proponent of thematic language learning, since it allows me to take a handful of words/concepts and reinforce them in a number of different ways. The clients still get the benefit of information repetition, much like one would get during a typical flashcard drill. However, they are also getting much more. Thematic language learning allows the client to increase word comprehension, make connections to real life scenarios, develop abstract thinking skills, as well as to transfer and generalize knowledge (Morrow, Pressley, Smith, & Smith, 1997; Ramey, 1995).
However, even though I dislike flashcards, I still don’t necessarily want to give up using them completely, especially because nowadays many different type of image based language flashcards can be found for free as both printables as well as Iphone/Ipad apps. Consequently, I decided to pick a free flashcard app and adapt it or rather “appdapt” it (coined by “The Speech Guy”, Jeremy Legaspi, the “Appdapt Guru”) in a meaningful and functional way for my students.
After looking over and rejecting a number of contenders, without a clear plan of action in mind, I stumbled upon a free app, ABA Flash Cards – Actions by kindergarten.com, which is designed to target verb labeling in ASD children. When I saw this app, I immediately knew how I wanted to appdapt it. I especially liked the fact that the app is made for both Ipad and Iphone. Here’s why.
My primary setting is an out of district day school inside a partial psychiatric hospital. So in my line of work I frequently do therapy with students just coming out from “chill out rooms” and “calm down areas”. This is definitely not the time when I want to bring or use a lot of materials in the session, since in a moment’s notice the session’s atmosphere can change from calm and productive into volatile and complicated. I also didn’t want to use a bulky Ipad in sessions with relatively new children on the caseload, since it usually takes a few sessions of careful observations and interaction to learn what makes them “tick”. Consequently, I was looking for an app which could ideally be downloaded onto not just the Ipad but also the Iphone. I reasoned that in unexpected situations I could simply put the phone into my pocket, unlike the Ipad, which in crisis situations can easily become a target or a missile.
Given the fact that many children with psychiatric disorders present with significant social pragmatic language deficits (Hyter, 2003; Hyter et al 2001; Cohen et al., 1998; Bryan, 1991; Goldman, 1987 ), which is certainly the case for the children on my caseload, I planned on adapting this app to target my students’ pragmatic language development, social problem solving skills as well as perspective taking abilities.
So here are just a few examples of how I appdapted the cards. First, I turned off the sound, since the visual images were what I was going after. Then I separated the cards into several categories and formulated some sample questions and scenarios that I was going to ask/pose to the students:
Making Inferences (re: People, Locations and Actions)

What do you think the girl is thinking about?
How do you know what she is thinking?
How do you think she is feeling?
How can you tell?
Where do you think she is?
How do you know?
Multiple Interpretations of Actions and Settings:

What do you think the girl is doing?
What else could she be doing?
 How does the boy feel about the flower?
How does the boy feel about the flower?
Give me a different explanation of how else can he possibly feel?

Who are the boys in the picture? (relationship)
Who else could they be?
What do you think the boy in a blue shirt is whispering to the boy in a red shirt?
What else could he be saying?
How do you know?
Supporting Empathy/Sympathy and Developing Peer Relatedness:

How does this child feel?
Why do you think he is crying?
What can you ask him/tell him to make things better?
 The girl is laughing because someone did something nice for her?
The girl is laughing because someone did something nice for her?
What do you think they did?
Interpreting Ambiguous Situations:

What is the girl doing?
Who do you think is the woman in the picture?
How do you know?
How does she feel about what the girl is doing?
How do you know?
My goal was to help the students how to correctly interpret facial features, body language, and context clues in order to teach them how to appropriately justify their responses. I also wanted to demonstrate to them that many times the situations in which we find ourselves in or the scenes that we are confronted with on daily basis could be interpreted in multiple ways. Moreover, I wanted to teach how appropriately speak to, console, praise, or compliment others in order to improve their ability to relate to peers. Finally, I wanted to provide them with an opportunity to improve their perspective taking abilities so they could comprehend and verbally demonstrate that other people could have feelings, beliefs and desires different from theirs.
Since I knew that many of my students had significant difficulties with even such simple tasks as labeling and identifying feelings, I also wanted to make sure that the students got multiple opportunities to describe a variety of emotions that they saw in the images, beyond offering the rudimentary labels of “happy”, “mad”, “sad”, so I took pictures of Emotions Word Bank as well as Emotion Color Wheel courtesy of the Do2Learn website, to store in my phone, in order to provide them with extra support.
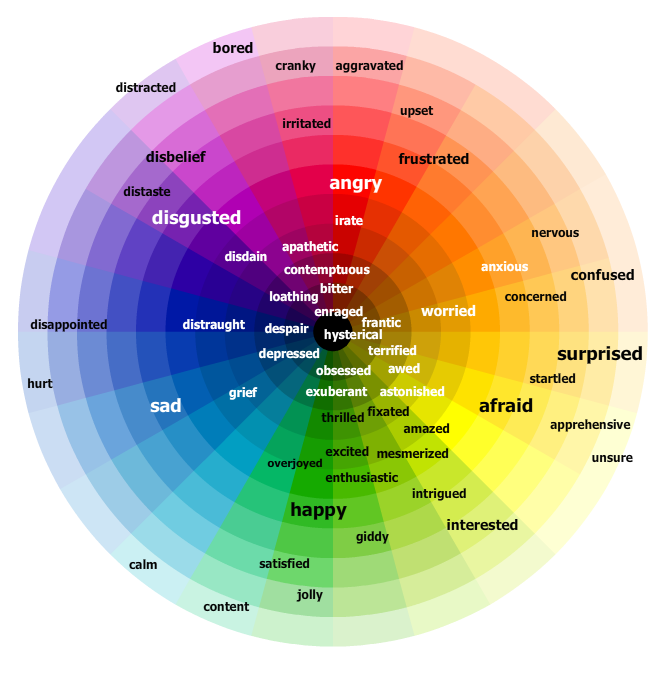

The above allowed me not only to provide them with visual and written illustrations but also to teach them synonyms and antonyms of relevant words. Finally, per my psychotherapist colleagues request, I also compiled a list of vocabulary terms reflecting additional internal states besides emotions (happy, mad) and emotional behaviors (laughing, crying, frowning). These included words related to: Cognition (know, think, remember, guess), Perception (see, hear, watch, feel), and Desire (want, need, wish), (Dodd, 2012) so my students could optimally benefit not just from language related therapy services but also their individual psychotherapy sessions as well.
I’ve only just began trialing the usage of this app with the students but I have to admit, even though its still the early days, so far things have been working pretty well. Looks like there’s hope for flashcards after all!
References:
Bryan, T. (1991). Social problems and learning disabilities. In B. Y. L. Wong (Ed.), Learning about learning disabilities (pp. 195-229). San Diego, CA: Academic Press.
Cohen, N. & Barwick, M. (1996) Comorbidity of Language and Social-Emotional Disorders: Comparison of Psychiatric Outpatients and Their Siblings. Journal of Clinical Child Psychology, 25(2), 192-200.
Goldman, L. G. (1987). Social implications of learning disorders. Reading, Writing and Learning Disabilities, 3, 119-130.
Hyter, Y. D., et al (2001). Pragmatic language intervention for children with language and emotional/behavioral disorders. Communication Disorders Quarterly, 23(1), 4–16.
Hyter, Y. D. (2003). Language intervention for children with emotional or behavioral disorders. Behavioral Disorders, 29, 65–76.
Morrow, L. M., Pressley, M., Smith, J.K., & Smith, M. (1997). The effect of a literature-based program integrated into literacy and science instruction with children from diverse background. Reading Research Quarterly, 32(1), 54-76.
Petersen, D. B., Dodd, J & Finestack, L. H (2012, Oct 9) Narrative Assessment and Intervention: Live Chat. Sponsored by SIG 1: Language Learning and Education. http://www.asha.org/events/live/10-09-2012-narrative-assessment-and-intervention/
Ramey, E. K. (1995). An integrated approach to language arts instruction. The Reading Teacher, 48(5), 418-419.
 Recently, I’ve published an article in SIG 16 Perspectives on School Based Issues discussing the importance of social communication assessments of school aged children 2-18 years of age. Below I would like to summarize article highlights.
Recently, I’ve published an article in SIG 16 Perspectives on School Based Issues discussing the importance of social communication assessments of school aged children 2-18 years of age. Below I would like to summarize article highlights. Graduation time is rapidly approaching and many graduate speech language pathology students are getting ready to begin their first days in the workforce. When it comes to juggling caseloads and managing schedules, time is money and efficiency is the key to success. Consequently, a few years ago I created SLP Efficiency Bundles™, which are materials highly useful for Graduate SLPs working with pediatric clients. These materials are organized by areas of focus for efficient and effective screening, assessment, and treatment of speech and language disorders.
Graduation time is rapidly approaching and many graduate speech language pathology students are getting ready to begin their first days in the workforce. When it comes to juggling caseloads and managing schedules, time is money and efficiency is the key to success. Consequently, a few years ago I created SLP Efficiency Bundles™, which are materials highly useful for Graduate SLPs working with pediatric clients. These materials are organized by areas of focus for efficient and effective screening, assessment, and treatment of speech and language disorders.  Frequently, I see a variation of the following scenario on many speech and language forums.
Frequently, I see a variation of the following scenario on many speech and language forums. Let’s begin by answering a few simple questions. Was a thorough language evaluation with an emphasis on the child’s social pragmatic language abilities been completed? And by thorough, I am not referring to general language tests but to a variety of formal and informal social pragmatic language testing (read more
Let’s begin by answering a few simple questions. Was a thorough language evaluation with an emphasis on the child’s social pragmatic language abilities been completed? And by thorough, I am not referring to general language tests but to a variety of formal and informal social pragmatic language testing (read more  Please note that none of the general language tests such as the Preschool Language Scale-5 (PLS-5), Comprehensive Assessment of Spoken Language (CASL-2), the Test of Language Development-4 (TOLD-4) or even the Clinical Evaluation of Language Fundamentals Tests (CELF-P2)/ (CELF-5) tap into the child’s social language competence because they do NOT directly test the child’s social language skills (e.g., CELF-5 assesses them via a parental/teachers questionnaire). Thus, many children can attain average scores on these tests yet still present with pervasive social language deficits. That is why it’s very important to thoroughly assess social pragmatic language abilities of all children (no matter what their age is) presenting with behavioral deficits.
Please note that none of the general language tests such as the Preschool Language Scale-5 (PLS-5), Comprehensive Assessment of Spoken Language (CASL-2), the Test of Language Development-4 (TOLD-4) or even the Clinical Evaluation of Language Fundamentals Tests (CELF-P2)/ (CELF-5) tap into the child’s social language competence because they do NOT directly test the child’s social language skills (e.g., CELF-5 assesses them via a parental/teachers questionnaire). Thus, many children can attain average scores on these tests yet still present with pervasive social language deficits. That is why it’s very important to thoroughly assess social pragmatic language abilities of all children (no matter what their age is) presenting with behavioral deficits.

 In March 2014,
In March 2014, 
 Inattentiveness, hyperactivity, and impulsivity are the most common presenting behavioral problems in at-risk children. This workshop will describe select speech language causes of hyperactivity and inattentiveness in children beyond the ADHD diagnosis, including traumatic brain injury, auditory processing disorders, severe language disorders, as well as social pragmatic language deficits.It will review case examples to illustrate the importance of differential diagnosis. Implications for assessment as well as the need for relevant referrals will be discussed.
Inattentiveness, hyperactivity, and impulsivity are the most common presenting behavioral problems in at-risk children. This workshop will describe select speech language causes of hyperactivity and inattentiveness in children beyond the ADHD diagnosis, including traumatic brain injury, auditory processing disorders, severe language disorders, as well as social pragmatic language deficits.It will review case examples to illustrate the importance of differential diagnosis. Implications for assessment as well as the need for relevant referrals will be discussed. This article was originally published in December 24, 2012 issue of Advance for Speech Language Pathologists and Audiologists under the title: “Adoption & Pragmatic Problems” (pp 6-9)
This article was originally published in December 24, 2012 issue of Advance for Speech Language Pathologists and Audiologists under the title: “Adoption & Pragmatic Problems” (pp 6-9) 



