 In the past several years there has been a sharp decline in international adoptions. Whereas in 2004, Americans adopted a record high of 22,989 children from overseas, in 2015, only 5,647 children (a record low in 30 years) were adopted from abroad by American citizens.
In the past several years there has been a sharp decline in international adoptions. Whereas in 2004, Americans adopted a record high of 22,989 children from overseas, in 2015, only 5,647 children (a record low in 30 years) were adopted from abroad by American citizens.
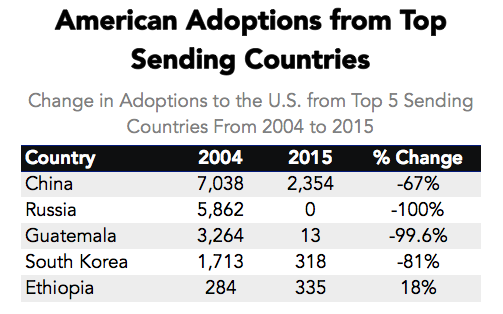
Primary Data Source: Data Source: U.S. State Department Intercountry Adoption Statistics
Secondary Data Source: Why Did International Adoption Suddenly End?
Despite a sharp decline in adoptions many SLPs still frequently continue to receive internationally adopted (IA) children for assessment as well as treatment – immediately post adoption as well as a number of years post-institutionalization.
In the age of social media, it may be very easy to pose questions and receive instantaneous responses on platforms such as Facebook and Twitter with respect to assessment and treatment recommendations. However, it is very important to understand that many SLPs, who lack direct clinical experience in international adoptions may chime in with inappropriate recommendations with respect to the assessment or treatment of these children.
Consequently, it is important to identify reputable sources of information when it comes to speech-language assessment of internationally adopted children.
There are a number of researchers in both US and abroad who specialize in speech-language abilities of Internationally Adopted children. This list includes (but is by far not limited to) the following authors:
- Boris Gindis
- Sharon Glennen
- Deborah Hwa-Froelich
- Kathleen A. Scott
- Jenny A. Roberts
- Karen E. Pollock
- M. Gay Masters
- Monica Dalen
The works of these researchers can be readily accessed in the ASHA Journals or via ResearchGate.
Meanwhile, here are some basic facts regarding internationally adopted children that all SLPs and parents need to know.
Demographics:
- A greater number of older, preschool and school-aged children and fewer number of infants and toddlers are placed for adoption (Selman, 2012).
- Significant increase in special needs adoptions from Eastern European countries (e.g., Ukraine, Kazhakstan, etc.) as well as China. The vast majority of Internationally Adopted children arrive to the United States with significant physical, linguistic, and cognitive disabilities as well as mental health problems. Consequently, it is important for schools to immediately provide the children with a host of services including speech-language therapy, immediately post-arrival.
- It is also important to know that in the vast majority of cases the child’s linguistic, cognitive, or mental health deficits may not be documented in the adoption records due to poor record keeping, lack of access to adequate healthcare or often to ensure their “adoptability”. As such, parental interviews and anecdotal evidence become the primary source of information regarding these children’s social and academic functioning in their respective birth countries.
The question of bilingualism:
- Internationally Adopted children are NOT bilingual children! In fact, the vast majority of internationally adopted children will very rapidly lose their birth language, in a period of 2-3 months post arrival (Gindis, 2005), since they are most often adopted by parents who do not speak the child’s birth language and as such are unable/unwilling to maintain it.
- IA children do not need to be placed in ESL classes since they are not bilingual children. Not only are IA children not bilingual, they are also not ‘truly’ monolingual since their first language is lost rather rapidly, while their second language has been gained minimally at the time of loss.
- IA children need to acquire Cognitive Language Mastery (CLM) which is language needed for formal academic learning. This includes listening, speaking, reading, and writing about subject area content material including analyzing, synthesizing, judging and evaluating presented information. This level of language learning is essential for a child to succeed in school. CLM takes years and years to master, especially because, IA children did not have the same foundation of knowledge and stimulation as bilingual children in their birth countries.

- IA children’s language abilities should be retested and monitored at regular intervals during the first several years post arrival.
- Glennen (2007) recommends 3 evaluations during the first year post arrival, with annual reevaluations thereafter.
- Hough & Kaczmarek (2011) recommend a reevaluation schedule of 3-4 times a year for a period of two years, post arrival because some IA children continue to present with language-based deficits many years (5+) post-adoption.
- If an SLP speaking the child’s first language is available the window of opportunity to assess in the first language is very limited (~2-3 months at most).
- Similarly, an assessment with an interpreter is recommended immediately post arrival from the birth country for a period of approximately the same time.
- If an SLP speaking the child’s first language is not available English-speaking SLP should consider assessing the child in English between 3-6 months post arrival (depending on the child and the situational constraints) in order to determine the speed with which s/he are acquiring English language abilities
- Children should be demonstrating rapid language gains in the areas of receptive language, vocabulary as well as articulation (Glennen 2007, 2009)
- Dynamic assessment is highly recommended
- It is important to remember that language and literacy deficits are not always very apparent and can manifest during any given period post arrival
To treat or NOT to Treat?
- “Any child with a known history of speech and language delays in the sending country should be considered to have true delays or disorders and should receive speech and language services after adoption.” (Glennen, 2009, p.52)
- IA children with medical diagnoses, which impact their speech language abilities should be assessed and considered for S-L therapy services as well (Ladage, 2009).
Helpful Links:
- Elleseff, T (2013) Changing Trends in International Adoption: Implications for Speech-Language Pathologists. Perspectives on Global Issues in Communication Sciences and Related Disorders, 3: 45-53
- Assessing Behaviorally Impaired Students: Why Background History Matters!
- Dear School Professionals Please Be Aware of This
- What parents need to know about speech-language assessment of older internationally adopted children
- Understanding the risks of social pragmatic deficits in post institutionalized internationally adopted (IA) children
- Understanding the extent of speech and language delays in older internationally adopted children
References:
- Gindis, B. (2005). Cognitive, language, and educational issues of children adopted from overseas orphanages. Journal of Cognitive Education and Psychology, 4 (3): 290-315.
- Glennen, S (2009) Speech and language guidelines for children adopted from abroad at older ages. Topics in language Disorders 29, 50-64.
- Ladage, J. S. (2009). Medical Issues in International Adoption and Their Influence on Language Development. Topics in Language Disorders , 29 (1), 6-17.
- Selman P. (2012) Global trends in Intercountry Adoption 2000-2010. New York: National Council for Adoption, 2012.
- Selman P. The global decline of intercountry adoption: What lies ahead?. Social Policy and Society 2012, 11(3), 381-397.
Additional Helpful References:
- Abrines, N., Barcons, N., Brun, C., Marre, D., Sartini, C., & Fumadó, V. (2012). Comparing ADHD symptom levels in children adopted from Eastern Europe and from other regions: discussing possible factors involved. Children and Youth Services Review, 34 (9) 1903-1908.
- Balachova, T et al (2010). Changing physicians’ knowledge, skills and attitudes to prevent FASD in Russia: 800. Alcoholism: Clinical & Experimental Research. 34(6) Sup 2:210A.
- Barcons-Castel, N, Fornieles-Deu,A, & Costas-Moragas, C (2011). International adoption: assessment of adaptive and maladaptive behavior of adopted minors in Spain. The Spanish Journal of Psychology, 14 (1): 123-132.
- Beverly, B., McGuinness, T., & Blanton, D. (2008). Communication challenges for children adopted from the former Soviet Union. Language, Speech, and Hearing Services in Schools, 39, 1-11.
- Cohen, N. & Barwick, M. (1996). Comorbidity of language and social-emotional disorders: comparison of psychiatric outpatients and their siblings. Journal of Clinical Child Psychology, 25(2), 192-200.
- Croft, C et al, (2007). Early adolescent outcomes of institutionally-deprived and nondeprived adoptees: II. Language as a protective factor and a vulnerable outcome. The Journal of Child Psychology and Psychiatry, 48, 31–44.
- Dalen, M. (2001). School performances among internationally adopted children in Norway. Adoption Quarterly, 5(2), 39-57.
- Dalen, M. (1995). Learning difficulties among inter-country adopted children. Nordisk pedagogikk, 15 (No. 4), 195-208
- Davies, J., & Bledsoe, J. (2005). Prenatal alcohol and drug exposures in adoption. Pediatric Clinics of North America, 52, 1369–1393.
- Desmarais, C., Roeber, B. J., Smith, M. E., & Pollak, S. D. (2012). Sentence comprehension in post-institutionalized school-age children. Journal of Speech, Language, and Hearing Research, 55, 45-54
- Eigsti, I. M., Weitzman, C., Schuh, J. M., de Marchena, A., & Casey, B. J. (2011). Language and cognitive outcomes in internationally adopted children. Development and Psychopathology, 23, 629-646.
- Geren, J., Snedeker, J., & Ax, L. (2005). Starting over: a preliminary study of early lexical and syntactic development in internationally-adopted preschoolers. Seminars in Speech & Language, 26:44-54.
- Gindis (2008) Abrupt native language loss in international adoptees. Advance for Speech/Language Pathologists and Audiologists. 18(51): 5.
- Gindis, B. (2005). Cognitive, language, and educational issues of children adopted from overseas orphanages. Journal of Cognitive Education and Psychology, 4 (3): 290-315. Gindis, B. (1999) Language-related issues for international adoptees and adoptive families. In: T. Tepper, L. Hannon, D. Sandstrom, Eds. “International Adoption: Challenges and Opportunities.” PNPIC, Meadow Lands , PA. , pp. 98-108
- Glennen, S (2009) Speech and language guidelines for children adopted from abroad at older ages. Topics in language Disorders 29, 50-64.
- Glennen, S. (2007) Speech and language in children adopted internationally at older ages. Perspectives on Communication Disorders in Culturally and Linguistically Diverse Populations, 14, 17–20.
- Glennen, S., & Bright, B. J. (2005). Five years later: language in school-age internally adopted children. Seminars in Speech and Language, 26, 86-101.
- Glennen, S. & Masters, G. (2002). Typical and atypical language development in infants and toddlers adopted from Eastern Europe. American Journal of Speech-Language Pathology, 44, 417-433
- Gordina, A (2009) Parent Handout: The Dream Referral, Unpublished Manuscript.
- Hough, S., & Kaczmarek, L. (2011). Language and reading outcomes in young children adopted from Eastern European orphanages. Journal of Early Intervention, 33, 51-57.
- Hwa-Froelich, D (2012) Childhood maltreatment and communication development. Perspectives on School-Based Issues, 13: 43-53;
- Jacobs, E., Miller, L. C., & Tirella, G. (2010). Developmental and behavioral performance of internationally adopted preschoolers: a pilot study. Child Psychiatry and Human Development, 41, 15–29.
- Jenista, J., & Chapman, D. (1987). Medical problems of foreign-born adopted children. American Journal of Diseases of Children, 141, 298–302.
- Johnson, D. (2000). Long-term medical issues in international adoptees. Pediatric Annals, 29, 234–241.
- Judge, S. (2003). Developmental recovery and deficit in children adopted from Eastern European orphanages. Child Psychiatry and Human Development, 34, 49–62.
- Krakow, R. A., & Roberts, J. (2003). Acquisitions of English vocabulary by young Chinese adoptees. Journal of Multilingual Communication Disorders, 1, 169-176
- Ladage, J. S. (2009). Medical issues in international adoption and their influence on language development. Topics in Language Disorders , 29 (1), 6-17.
- Loman, M. M., Wiik, K. L., Frenn, K. A., Pollak, S. D., & Gunnar, M. R. (2009). Post-institutionalized children’s development: growth, cognitive, and language outcomes. Journal of Developmental Behavioral Pediatrics, 30, 426–434.
- McLaughlin, B., Gesi Blanchard, A., & Osanai, Y. (1995). Assessing language development in bilingual preschool children. Washington, D.C.: National Clearinghouse for Bilingual Education.
- Miller, L., Chan, W., Litvinova, A., Rubin, A., Tirella, L., & Cermak, S. (2007). Medical diagnoses and growth of children residing in Russian orphanages. Acta Paediatrica, 96, 1765–1769.
- Miller, L., Chan, W., Litvinova, A., Rubin, A., Comfort, K., Tirella, L., et al. (2006). Fetal alcohol spectrum disorders in children residing in Russian orphanages: A phenotypic survey. Alcoholism: Clinical and Experimental Research, 30, 531–538.
- Miller, L. (2005). Preadoption counseling and evaluation of the referral. In L. Miller (Ed.), The Handbook of International Adoption Medicine (pp. 67-86). NewYork: Oxford.
- Pollock, K. E. (2005) Early language growth in children adopted from China: preliminary normative data. Seminars in Speech and Language, 26, 22-32.
- Roberts, J., Pollock, K., Krakow, R., Price, J., Fulmer, K., & Wang, P. (2005). Language development in preschool-aged children adopted from China. Journal of Speech, Language, and Hearing Research, 48, 93–107.
- Scott, K.A., Roberts, J.A., & Glennen, S. (2011). How well children who are internationally do adopted acquire language? A meta-analysis. Journal of Speech, Language and Hearing Research, 54. 1153-69.
- Scott, K.A., & Roberts, J. (2011). Making evidence-based decisions for children who are internationally adopted. Evidence-Based Practice Briefs. 6(3), 1-16.
- Scott, K.A., & Roberts, J. (2007) language development of internationally adopted children: the school-age years. Perspectives on Communication Disorders in Culturally and Linguistically Diverse Populations, 14: 12-17.
- Selman P. (2012a) Global trends in intercountry adoption 2000-2010. New York: National Council for Adoption.
- Selman P (2012b). The rise and fall of intercountry adoption in the 21st century. In: Gibbons, J.L., Rotabi, K.S, ed. Intercountry Adoption: Policies, Practices and Outcomes. London: Ashgate Press.
- Selman, P. (2010) “Intercountry adoption in Europe 1998–2009: patterns, trends and issues,” Adoption & Fostering, 34 (1): 4-19.
- Silliman, E. R., & Scott, C. M. (2009). Research-based oral language intervention routes to the academic language of literacy: Finding the right road. In S. A. Rosenfield & V. Wise Berninger (Eds.), Implementing evidence-based academic interventions in school (pp. 107–145). New York: Oxford University Press.
- Tarullo, A. R., Bruce, J., & Gunnar, M. (2007). False belief and emotion understanding in post-institutionalized children. Social Development, 16, 57-78
- Tarullo, A. & Gunnar, M. R. (2005). Institutional rearing and deficits in social relatedness: Possible mechanisms and processes. Cognitie, Creier, Comportament [Cognition, Brain, Behavior], 9, 329-342.
- Varavikova, E. A. & Balachova, T. N. (2010). Strategies to implement physician training in FAS prevention as a part of preventive care in primary health settings: P120.Alcoholism: Clinical & Experimental Research. 34(8) Sup 3:119A.
- Welsh, J. A., & Viana, A. G. (2012). Developmental outcomes of children adopted internationally. Adoption Quarterly, 15, 241-264.
 “Well, the school did their evaluations and he doesn’t qualify for services” tells me a parent of a 3.5 year old, newly admitted private practice client. “I just don’t get it” she says bemusedly, “It is so obvious to anyone who spends even 10 minutes with him that his language is nowhere near other kids his age!” “How can this happen?” she asks frustratedly?
“Well, the school did their evaluations and he doesn’t qualify for services” tells me a parent of a 3.5 year old, newly admitted private practice client. “I just don’t get it” she says bemusedly, “It is so obvious to anyone who spends even 10 minutes with him that his language is nowhere near other kids his age!” “How can this happen?” she asks frustratedly?


 As per NJAC 6A:14-2.5
As per NJAC 6A:14-2.5  These delays can be receptive (listening) or expressive (speaking) and need not be based on a total test score but rather on all testing findings with a minimum of at least two assessments being performed. A determination of adverse impact in academic and non-academic areas (e.g., social functioning) needs to take place in order for special education and related services be provided. Additionally, a delay in articulation can serve as a basis for consideration of eligibility as well.
These delays can be receptive (listening) or expressive (speaking) and need not be based on a total test score but rather on all testing findings with a minimum of at least two assessments being performed. A determination of adverse impact in academic and non-academic areas (e.g., social functioning) needs to take place in order for special education and related services be provided. Additionally, a delay in articulation can serve as a basis for consideration of eligibility as well. General Language:
General Language:  Pragmatics/Social Communication
Pragmatics/Social Communication Finally, by showing children simple
Finally, by showing children simple  Today I’d like to officially introduce a new
Today I’d like to officially introduce a new  Today I’d like to officially introduce a new
Today I’d like to officially introduce a new 



 Today I am very excited to introduce my new product “
Today I am very excited to introduce my new product “{kind=link}