 Today, I’d like to talk about speech and language assessments of children under three years of age. Namely, the quality of these assessments. Let me be frank, I am not happy with what I am seeing. Often times, when I receive a speech-language report on a child under three years of age, I am struck by how little functional information it contains about the child’s linguistic strengths and weaknesses. Indeed, conversations with parents often reveal that at best the examiner spent no more than half an hour or so playing with the child and performed very limited functional testing of their actual abilities. Instead, they interviewed the parent and based their report on parental feedback alone. Consequently, parents often end up with a report of very limited value, which does not contain any helpful information on how delayed is the child as compared to peers their age.
Today, I’d like to talk about speech and language assessments of children under three years of age. Namely, the quality of these assessments. Let me be frank, I am not happy with what I am seeing. Often times, when I receive a speech-language report on a child under three years of age, I am struck by how little functional information it contains about the child’s linguistic strengths and weaknesses. Indeed, conversations with parents often reveal that at best the examiner spent no more than half an hour or so playing with the child and performed very limited functional testing of their actual abilities. Instead, they interviewed the parent and based their report on parental feedback alone. Consequently, parents often end up with a report of very limited value, which does not contain any helpful information on how delayed is the child as compared to peers their age.
So today I like to talk about what information should such speech-language reports should contain. For the purpose of this particular post, I will choose a particular developmental age at which children at risk of language delay are often assessed by speech-language pathologists. Below you will find what information I typically like to include in these reports as well as developmental milestones for children 30 months or 2.5 years of age.
 Why 30 months, you may ask? Well, there isn’t really any hard science to it. It’s just that I noticed that a significant percentage of parents who were already worried about their children’s speech-language abilities when they were younger, begin to act upon those worries as the child is nearing 3 years of age and their abilities are not improving or are not commensurate with other peers their age.
Why 30 months, you may ask? Well, there isn’t really any hard science to it. It’s just that I noticed that a significant percentage of parents who were already worried about their children’s speech-language abilities when they were younger, begin to act upon those worries as the child is nearing 3 years of age and their abilities are not improving or are not commensurate with other peers their age.
So here is the information I include in such reports (after I’ve gathered pertinent background information in the form of relevant intakes and questionnaires, of course). Naturally, detailed BACKGROUND HISTORY section is a must! Prenatal, perinatal, and postnatal development should be prominently featured there. All pertinent medical history needs to get documented as well as all of the child’s developmental milestones in the areas of cognition, emotional development, fine and gross motor function, and of course speech and language. Here, I also include a family history of red flags: international or domestic adoption of the child (if relevant) as well as familial speech and language difficulties, intellectual impairment, psychiatric disorders, special education placements, or documented deficits in the areas of literacy (e.g., reading, writing, and spelling). After all, if any of the above issues are present in isolation or in combination, the risk for language and literacy deficits increases exponentially, and services are strongly merited for the child in question.
For bilingual children, the next section will cover LANGUAGE BACKGROUND AND USE. Here, I describe how many and which languages are spoken in the home and how well does the child understand and speak any or all of these languages (as per parental report based on questionnaires).
After that, I move on to describe the child’s ADAPTIVE BEHAVIOR during the assessment. In this section, I cover emotional relatedness, joint attention, social referencing, attention skills, communicative frequency, communicative intent, communicative functions, as well as any and all unusual behaviors noted during the therapy session (e.g., refusal, tantrums, perseverations, echolalia, etc.) Then I move on to PLAY SKILLS. For the purpose of play assessment, I use the Revised Westby Play Scale (Westby, 2000). In this section, I describe where the child is presently with respect to play skills, and where they actually need to be developmentally (excerpt below).
“During today’s assessment, LS’s play skills were judged to be significantly reduced for his age. A child of LS’s age (30 months) is expected to engage in a number of isolated pretend play activities with realistic props to represent daily experiences (playing house) as well as less frequently experienced events (e.g., reenacting a doctor’s visit, etc.) (corresponds to Stage VI on the Westby Play Scale, Revised Westby Play Scale (Westby, 2000)). Contrastingly, LS presented with limited repertoire routines, which were characterized primarily by exploration of toys, such as operating simple cause and effect toys (given modeling) or taking out and then putting back in playhouse toys. LS’s parents confirmed that the above play schemas were representative of play interactions at home as well. Today’s LS’s play skills were judged to be approximately at Stage II (13 – 17 months) on the Westby Play Scale, (Revised Westby Play Scale (Westby, 2000)) which is significantly reduced for a child of LS’s age, since it is almost approximately ±15 months behind his peers. Thus, based on today’s play assessment, LS’s play skills require therapeutic intervention. “
Sections on AUDITORY FUNCTION, PERIPHERAL ORAL MOTOR EXAM, VOCAL PARAMETERS, FLUENCY AND RESONANCE (and if pertinent FEEDING and SWALLOWING follow) (more on that in another post).
Now, it’s finally time to get to the ‘meat and potatoes’ of the report ARTICULATION AND PHONOLOGY as well as RECEPTIVE and EXPRESSIVE LANGUAGE (more on PRAGMATIC ASSESSMENT in another post).
First, here’s what I include in the ARTICULATION AND PHONOLOGY section of the report.
- Phonetic inventory: all the sounds the child is currently producing including (short excerpt below):
- Consonants: plosive (/p/, /b/, /m/), alveolar (/t/, /d/), velar (/k/, /g/), glide (/w/), nasal (/n/, /m/) glottal (/h/)
- Vowels and diphthongs: ( /a/, /e/, /i/, /o/, /u/, /ou/, /ai/)
- Phonotactic repertoire: What type of words comprised of how many syllables and which consonant-vowel variations the child is producing (excerpt below)
- LS primarily produced one syllable words consisting of CV (e.g., ke, di), CVC (e.g., boom), VCV (e.g., apo) syllable shapes, which is reduced for a child his age.
- Speech intelligibility in known and unknown contexts
- Phonological processes analysis
Now that I have described what the child is capable of speech-wise, I discuss where the child needs to be developmentally:
“A child of LS’s age (30 months) is expected to produce additional consonants in initial word position (k, l, s, h), some consonants (t, d, m, n, s, z) in final word position (Watson & Scukanec, 1997b), several consonant clusters (pw, bw, -nd, -ts) (Stoel-Gammon, 1987) as well as evidence a more sophisticated syllable shape structure (e.g., CVCVC) Furthermore, a 30 month old child is expected to begin monitoring and repairing own utterances, adjusting speech to different listeners, as well as practicing sounds, words, and early sentences (Clark, adapted by Owens, 1996, p. 386) all of which LS is not performing at this time. Based on above developmental norms, LS’s phonological abilities are judged to be significantly below age-expectancy at this time. Therapy is recommended in order to improve LS’s phonological skills.”
 At this point, I am ready to move on to the language portion of the assessment. Here it is important to note that a number of assessments for toddlers under 3 years of age contain numerous limitations. Some such as REEL-3 or Rosetti (a criterion-referenced vs. normed-referenced instrument) are observational or limitedly interactive in nature, while others such as PLS-5, have a tendency to over inflate scores, resulting in a significant number of children not qualifying for rightfully deserved speech-language therapy services. This is exactly why it’s so important that SLPs have a firm knowledge of developmental milestones! After all, after they finish describing what the child is capable of, they then need to describe what the developmental expectations are for a child this age (excerpts below).
At this point, I am ready to move on to the language portion of the assessment. Here it is important to note that a number of assessments for toddlers under 3 years of age contain numerous limitations. Some such as REEL-3 or Rosetti (a criterion-referenced vs. normed-referenced instrument) are observational or limitedly interactive in nature, while others such as PLS-5, have a tendency to over inflate scores, resulting in a significant number of children not qualifying for rightfully deserved speech-language therapy services. This is exactly why it’s so important that SLPs have a firm knowledge of developmental milestones! After all, after they finish describing what the child is capable of, they then need to describe what the developmental expectations are for a child this age (excerpts below).
RECEPTIVE LANGUAGE
“LS’s receptive language abilities were judged to be scattered between 11-17 months of age (as per clinical observations as well as informal PLS-5 and REEL-3 findings), which is also consistent with his play skills abilities (see above). During the assessment LS was able to appropriately understand prohibitive verbalizations (e.g., “No”, “Stop”), follow simple 1 part directions (when repeated and combined with gestures), selectively attend to speaker when his name was spoken (behavioral), perform a routine activity upon request (when combined with gestures), retrieve familiar objects from nearby (when provided with gestures), identify several major body parts (with prompting) on a doll only, select a familiar object when named given repeated prompting, point to pictures of familiar objects in books when named by adult, as well as respond to yes/no questions by using head shakes and head nods. This is significantly below age-expectancy.
A typically developing child 30 months of age is expected to spontaneously follow (without gestures, cues or prompts) 2+ step directives, follow select commands that require getting objects out of sight, answer simple “wh” questions (what, where, who), understand select spatial concepts, (in, off, out of, etc), understand select pronouns (e.g., me, my, your), identify action words in pictures, understand concept sizes (‘big’, ‘little’), identify simple objects according to their function, identify select clothing items such as shoes, shirt, pants, hat (on self or caregiver) as well as understand names of farm animals, everyday foods, and toys. Therapeutic intervention is recommended in order to increase LS’s receptive language abilities.
EXPRESSIVE LANGUAGE:
“During today’s assessment, LS’s expressive language skills were judged to be scattered between 10-15 months of age (as per clinical observations as well as informal PLS-5 and REEL-3 findings). LS was observed to communicate primarily via proto-imperative gestures (requesting and object via eye gaze, reaching) as well as proto-declarative gestures (showing an object via eye gaze, reaching, and pointing). Additionally, LS communicated via vocalizations, head nods, and head shakes. According to parental report, at this time LS’s speaking vocabulary consists of approximately 15-20 words (see word lists below). During the assessment LS was observed to spontaneously produce a number of these words when looking at a picture book, playing with toys, and participating in action based play activities with Mrs. S and clinician. LS was also observed to produce a number of animal sounds when looking at select picture books and puzzles. For therapy planning purposes, it is important to note that LS was observed to imitate more sounds and words, when they were supported by action based play activities (when words and sounds were accompanied by a movement initiated by clinician and then imitated by LS). Today LS was observed to primarily communicate via a very limited number of imitated and spontaneous one word utterances that labeled basic objects and pictures in his environment, which is significantly reduced for his age.
A typically developing child of LS’s chronological age (30 months) is expected to possess a minimum vocabulary of 200+ words (Rescorla, 1989), produce 2-4 word utterance combinations (e.g., noun + verb, verb + noun + location, verb + noun + adjective, etc), in addition to asking 2-3 word questions as well as maintaining a topic for 2+ conversational turns. Therapeutic intervention is recommended in order to increase LS’s expressive language abilities.”
Here you have a few speech-language evaluation excerpts which describe not just what the child is capable of but where the child needs to be developmentally. Now it’s just a matter of summarizing my IMPRESSIONS (child’s strengths and needs), RECOMMENDATIONS as well as SUGGESTED (long and short term) THERAPY GOALS. Now the parents have some understanding regarding their child’s strengths and needs. From here, they can also track their child’s progress in therapy as they now have some idea to what it can be compared to.
 Now I know that many of you will tell me, that this is a ‘perfect world’ evaluation conducted by a private therapist with an unlimited amount of time on her hands. And to some extent, many of you will be right! Yes, such an evaluation was a result of more than 30 minutes spent face-to-face with the child. All in all, it took probably closer to 90 minutes of face to face time to complete it and a few hours to write. And yes, this is a luxury only a few possess and many therapists in the early intervention system lack. But in the long run, such evaluations pay dividends not only, obviously, to your clients but to SLPs who perform them. They enhance and grow your reputation as an evaluating therapist. They even make sense from a business perspective. If you are well-known and highly sought after due to your evaluating expertise, you can expect to be compensated for your time, accordingly. This means that if you decide that your time and expertise are worth private pay only (due to poor insurance reimbursement or low EI rates), you can be sure that parents will learn to appreciate your thoroughness and will choose you over other providers.
Now I know that many of you will tell me, that this is a ‘perfect world’ evaluation conducted by a private therapist with an unlimited amount of time on her hands. And to some extent, many of you will be right! Yes, such an evaluation was a result of more than 30 minutes spent face-to-face with the child. All in all, it took probably closer to 90 minutes of face to face time to complete it and a few hours to write. And yes, this is a luxury only a few possess and many therapists in the early intervention system lack. But in the long run, such evaluations pay dividends not only, obviously, to your clients but to SLPs who perform them. They enhance and grow your reputation as an evaluating therapist. They even make sense from a business perspective. If you are well-known and highly sought after due to your evaluating expertise, you can expect to be compensated for your time, accordingly. This means that if you decide that your time and expertise are worth private pay only (due to poor insurance reimbursement or low EI rates), you can be sure that parents will learn to appreciate your thoroughness and will choose you over other providers.
So, how about it? Can you give it a try? Trust me, it’s worth it!
Selected References:
- Owens, R. E. (1996). Language development: An introduction (4th ed.). Boston, MA: Allyn & Bacon.
- Rescorla, L. (1989). The Language Development Survey: A screening tool for delayed language in toddlers. Journal of Speech and Hearing Disorders, 54, 587–599.
- Selby, J. C., Robb, M. P., & Gilbert, H. R. (2000). Normal vowel articulations between 15 and 36 months of age. Clinical Linguistics and Phonetics, 14, 255-266.
- Stoel-Gammon, C. (1987). Phonological skills of 2-year-olds. Language, Speech, and Hearing Services in Schools, 18, 323-329.
- Watson, M. M., & Scukanec, G. P. (1997b). Profiling the phonological abilities of 2-year-olds: A longitudinal investigation. Child Language Teaching and Therapy, 13, 3-14.
For more information on EI Assessments click on any of the below posts:
- Part II: Early Intervention Evaluations PART II: Assessing Suspected Motor Speech Disorders in Children Under 3
- Part III: Early Intervention Evaluations PART III: Assessing Children Under 2 Years of Age
- Part IV: Early Intervention Evaluations PART IV:Assessing Social Pragmatic Abilities of Children Under 3
 In recent years there has been an increase in research on the subject of diagnosis and treatment of Auditory Processing Disorders (APD), formerly known as Central Auditory Processing Disorders or CAPD.
In recent years there has been an increase in research on the subject of diagnosis and treatment of Auditory Processing Disorders (APD), formerly known as Central Auditory Processing Disorders or CAPD. Today it is my pleasure and privilege to interview 3 Australian lactation consultations: Lois Wattis, Renee Kam, and Pamela Douglas, the authors of a March 2017 article in the Breastfeeding Review: “Three experienced lactation consultants reflect upon the oral tie phenomenon” (which can be found
Today it is my pleasure and privilege to interview 3 Australian lactation consultations: Lois Wattis, Renee Kam, and Pamela Douglas, the authors of a March 2017 article in the Breastfeeding Review: “Three experienced lactation consultants reflect upon the oral tie phenomenon” (which can be found  Presently, systematic reviews1-3 demonstrate there is insufficient evidence for the above. However, when many professionals including myself, cite reputable research explaining the lack of support of surgical intervention for tongue tie, there has been a pushback on the part of a number of other health professionals including lactation consultants, nurses, dentists, as well as speech-language pathologists stating that in their clinical experience surgical intervention does resolve issues with tongue tie as related to speech and feeding.
Presently, systematic reviews1-3 demonstrate there is insufficient evidence for the above. However, when many professionals including myself, cite reputable research explaining the lack of support of surgical intervention for tongue tie, there has been a pushback on the part of a number of other health professionals including lactation consultants, nurses, dentists, as well as speech-language pathologists stating that in their clinical experience surgical intervention does resolve issues with tongue tie as related to speech and feeding.
 Pamela Douglas:
Pamela Douglas: 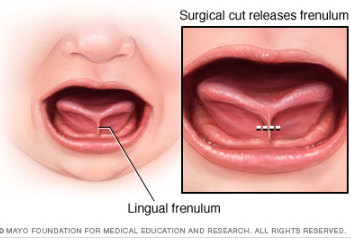
 Tatyana Elleseff: Thank you! This is highly relevant information for both health professionals and parents alike. I truly appreciate your clinical expertise on this topic. While we are on the topic of restrictive lingual frenulums can we discuss several recent articles published on surgical interventions for the above? For example (Ghaheri, Cole, Fausel, Chuop & Mace, 2016), recently published the result of their study which concluded that: “Surgical release of tongue-tie/lip-tie results in significant improvement in breastfeeding outcomes”. Can you elucidate upon the study design and its findings?
Tatyana Elleseff: Thank you! This is highly relevant information for both health professionals and parents alike. I truly appreciate your clinical expertise on this topic. While we are on the topic of restrictive lingual frenulums can we discuss several recent articles published on surgical interventions for the above? For example (Ghaheri, Cole, Fausel, Chuop & Mace, 2016), recently published the result of their study which concluded that: “Surgical release of tongue-tie/lip-tie results in significant improvement in breastfeeding outcomes”. Can you elucidate upon the study design and its findings? Tatyana Elleseff: Thank you for that. In addition to studies on tongue tie revisions and breastfeeding outcomes, there has been an increase in studies, specifically Kotlow (2016) and Siegel (2016), which claimed that surgical intervention improves outcomes for acid reflux and aerophagia in babies”. Can you discuss these studies design and findings?
Tatyana Elleseff: Thank you for that. In addition to studies on tongue tie revisions and breastfeeding outcomes, there has been an increase in studies, specifically Kotlow (2016) and Siegel (2016), which claimed that surgical intervention improves outcomes for acid reflux and aerophagia in babies”. Can you discuss these studies design and findings? There you have it, readers. Both research and clinical practice align to indicate that:
There you have it, readers. Both research and clinical practice align to indicate that: Since many children with restricted frenulum do not have any speech production difficulties, Dr Kummer explains why that is the case by discussing
Since many children with restricted frenulum do not have any speech production difficulties, Dr Kummer explains why that is the case by discussing 



 High comorbidity between language and psychiatric disorders has been well documented (Beitchman, Cohen, Konstantaras, & Tannock, 1996; Cohen, Barwick, Horodezky, Vallence, & Im, 1998; Toppelberg & Shapiro, 2000). However, a lesser known fact is that there’s also a significant under-diagnosis of language impairments in children with psychiatric disorders.
High comorbidity between language and psychiatric disorders has been well documented (Beitchman, Cohen, Konstantaras, & Tannock, 1996; Cohen, Barwick, Horodezky, Vallence, & Im, 1998; Toppelberg & Shapiro, 2000). However, a lesser known fact is that there’s also a significant under-diagnosis of language impairments in children with psychiatric disorders. 






 As an SLP who routinely conducts speech and language assessments in several settings (e.g., school and private practice), I understand the utility of and the need for standardized speech, language, and literacy tests. However, as an SLP who works with children with dramatically varying degree of cognition, abilities, and skill-sets, I also highly value supplementing these standardized tests with functional and dynamic assessments, interactions, and observations.
As an SLP who routinely conducts speech and language assessments in several settings (e.g., school and private practice), I understand the utility of and the need for standardized speech, language, and literacy tests. However, as an SLP who works with children with dramatically varying degree of cognition, abilities, and skill-sets, I also highly value supplementing these standardized tests with functional and dynamic assessments, interactions, and observations. Since a significant value is placed on standardized testing by both schools and insurance companies for the purposes of service provision and reimbursement, I wanted to summarize in today’s post the findings of recent articles on this topic. Since my primary interest lies in assessing and treating school-age children, for the purposes of today’s post all of the reviewed articles came directly from the
Since a significant value is placed on standardized testing by both schools and insurance companies for the purposes of service provision and reimbursement, I wanted to summarize in today’s post the findings of recent articles on this topic. Since my primary interest lies in assessing and treating school-age children, for the purposes of today’s post all of the reviewed articles came directly from the  Turns out it did not! Turns out due to the variation in psychometric properties of various tests (
Turns out it did not! Turns out due to the variation in psychometric properties of various tests (
 Thus they urged SLPs to exercise caution in determining the severity of children’s language impairment via norm-referenced test performance “given the inconsistency in guidelines and lack of empirical data within test manuals to support this use (176)”.
Thus they urged SLPs to exercise caution in determining the severity of children’s language impairment via norm-referenced test performance “given the inconsistency in guidelines and lack of empirical data within test manuals to support this use (176)”. But are the SLPs from across the country appropriately using the federal and state guidelines in order to determine eligibility?
But are the SLPs from across the country appropriately using the federal and state guidelines in order to determine eligibility? So where do we go from here? Well, it’s quite simple really! We already know what the problem is. Based on the above articles we know that:
So where do we go from here? Well, it’s quite simple really! We already know what the problem is. Based on the above articles we know that: In my therapy sessions I spend a significant amount of time improving literacy skills (reading, spelling, and writing) of language impaired students. In my work with these students I emphasize goals with a focus on phonics, phonological awareness, encoding (spelling) etc. However, what I have frequently observed in my sessions are significant gaps in the students’ foundational knowledge pertaining to the basics of sound production and letter recognition. Basic examples of these foundational deficiencies involve students not being able to fluently name the letters of the alphabet, understand the difference between vowels and consonants, or fluently engage in sound/letter correspondence tasks (e.g., name a letter and then quickly and accurately identify which sound it makes). Consequently, a significant portion of my sessions involves explicit instruction of the above concepts.
In my therapy sessions I spend a significant amount of time improving literacy skills (reading, spelling, and writing) of language impaired students. In my work with these students I emphasize goals with a focus on phonics, phonological awareness, encoding (spelling) etc. However, what I have frequently observed in my sessions are significant gaps in the students’ foundational knowledge pertaining to the basics of sound production and letter recognition. Basic examples of these foundational deficiencies involve students not being able to fluently name the letters of the alphabet, understand the difference between vowels and consonants, or fluently engage in sound/letter correspondence tasks (e.g., name a letter and then quickly and accurately identify which sound it makes). Consequently, a significant portion of my sessions involves explicit instruction of the above concepts. So I do! Furthermore, I can tell you that explicit instruction of metalinguistic vocabulary does significantly improve my students understanding of the tasks involved in obtaining literacy competence. Even my students with mild to moderate intellectual disabilities significantly benefit from understanding the meanings of: letters, words, sentences, etc.
So I do! Furthermore, I can tell you that explicit instruction of metalinguistic vocabulary does significantly improve my students understanding of the tasks involved in obtaining literacy competence. Even my students with mild to moderate intellectual disabilities significantly benefit from understanding the meanings of: letters, words, sentences, etc. A word of caution as though regarding using
A word of caution as though regarding using 

 As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.
As a speech language pathologist (SLP) who works in an outpatient psychiatric school-based setting, I frequently review incoming students previous speech language evaluation reports. There are a number of trends I see in these reports which I have written about in the past as well as planned on writing about in the future.





{kind=link}